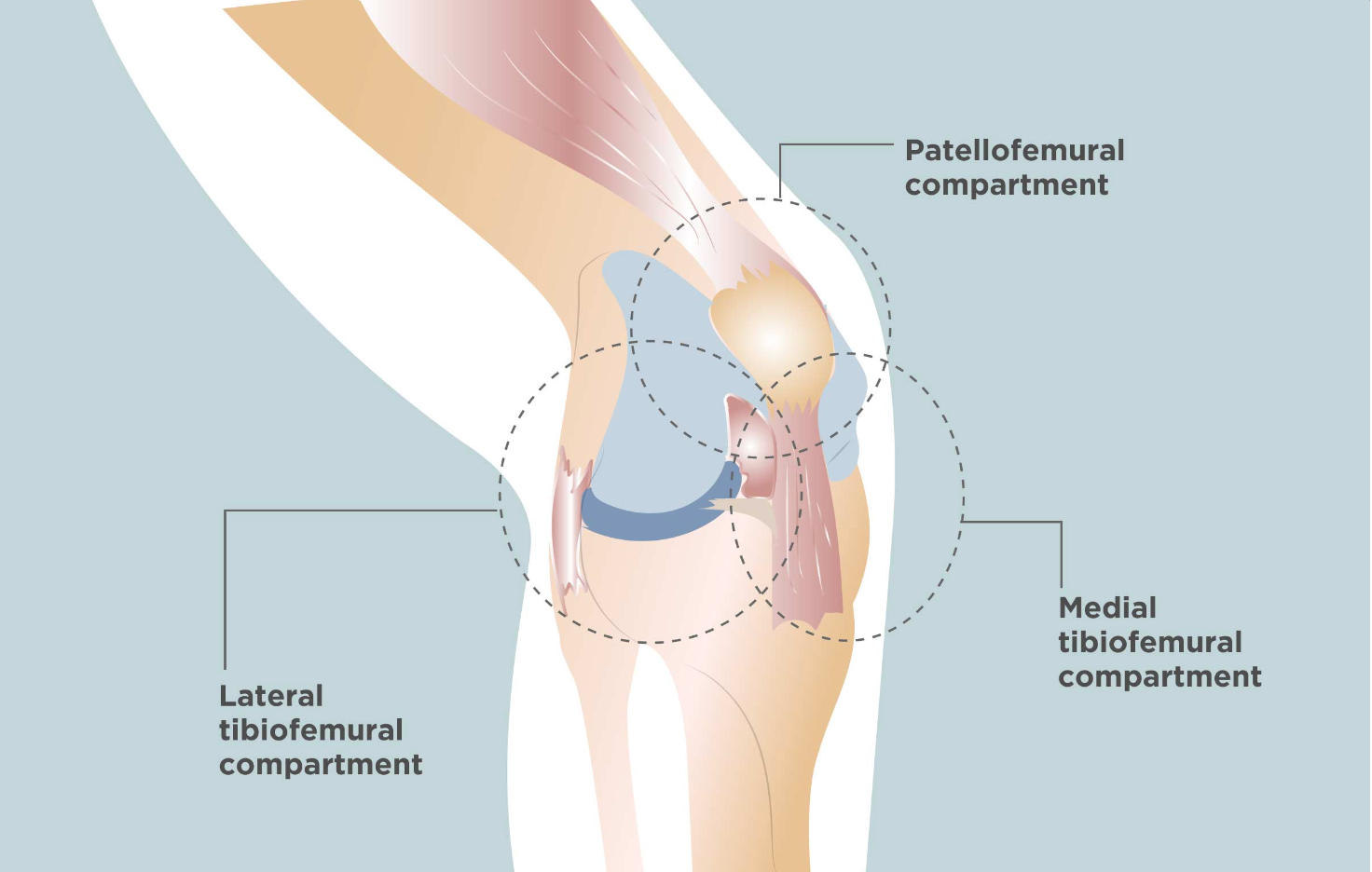
The knee is anatomically divided into three compartments: the patellofemoral, medial, and lateral compartments. The patellofemoral compartment is situated at the front of the knee, between the patella (kneecap) and the lower femur (thigh bone). The medial compartment is located on the inner side of the knee, while the lateral compartment is found on the outer side of the knee joint. Patellofemoral instability refers to a condition where the patella (kneecap) moves out of its normal alignment pattern. This misalignment can lead to damage of the surrounding soft tissues, including muscles and ligaments responsible for knee stability, as well as the articular cartilage of the patella and femoral trochlea.
Patellofemoral instability can arise due to variations in the shape of the patella or its trochlear groove during knee bending and straightening. Typically, the patella moves within the trochlear groove as the knee flexes or extends. However, instability occurs when the patella partially (subluxation) or completely (dislocation) moves out of this groove. Several factors can contribute to this abnormal tracking, including anatomical defects such as flat feet or congenital abnormalities in patella or femoral trochlea shape. An abnormal Q angle, particularly high Q angle, seen in individuals with knock knees, can also lead to patellar misalignment. Additionally, patellofemoral arthritis resulting from abnormal patellar tracking can cause loss of articular cartilage on the patella's back and subsequent arthritis. Muscle imbalance, particularly weak quadriceps muscles, can further exacerbate patellar tracking issues, increasing the risk of lateral subluxation or dislocation. This condition is more common in young, active individuals involved in sports activities.
Patellofemoral instability commonly presents with pain upon standing up from a sitting position and a sensation that the knee may buckle or give way. In cases where the kneecap partially or completely slips out of place, individuals may experience severe pain, swelling, bruising, visible deformity, and loss of knee function. Additionally, sensory changes such as numbness or partial paralysis below the dislocation may occur due to pressure on nerves and blood vessels.
The diagnosis of patellofemoral instability typically involves a combination of the patient's medical history, a thorough clinical examination, and appropriate investigations. Knee X-rays taken from various angles provide insights into the patellofemoral joint's position, any changes in patellar alignment or tilt, as well as instances of patellar subluxation or dislocation. Additionally, X-rays can reveal abnormalities in the femoral trochlea, such as shallow grooves. MRI scans are valuable for assessing the condition of the articular cartilage in the patella and knee joint, as well as detecting any patellar malalignment or injuries to the patellofemoral ligaments. In some cases, a CT scan may be performed to explore potential underlying causes of patellofemoral instability, with 3D reconstruction aiding in the assessment of joint alignment and severity of any malalignment present.
Patients experiencing patellofemoral instability, characterized by misalignment of the patella, require treatment to restore normal patellar alignment. Treatment approaches, whether conservative or surgical, are determined based on clinical examination and investigation findings. Conservative treatment is typically recommended for cases of patellar subluxation (partial dislocation). This may include the use of pain relievers, rest from strenuous activities, application of ice or warm compresses, and physiotherapy aimed at strengthening the quadriceps muscles and improving patellar tracking. Various taping techniques may also be utilized to enhance or maintain patellar alignment. In instances of complete patellar dislocation, closed reduction under anesthesia may be necessary to relocate the patella within the femoral trochlear groove. Additionally, specialized knee braces may be employed to maintain reduced patellar alignment. Surgical intervention may be considered when conservative measures fail to restore normal patellar tracking. The goal of surgery is to realign the patella within the groove and reduce the Q angle. The choice of surgical procedure is determined by clinical evaluation and investigation findings. Patellar realignment surgery is broadly classified into proximal and distal re-alignment procedures, which may be performed individually or in combination. Proximal re-alignment procedures involve lengthening structures limiting patellar movement on the outside (lateral release) or shortening ligaments on the inside (medial plication) of the patella. In cases of femoral groove malformation or shallowness, femoral trochleoplasty may be performed. Distal re-alignment procedures aim to decrease the Q angle, often through tibial tubercle transfer (TTT), where the tibial tubercle with its attached patellar tendon is repositioned to the medial portion of the upper tibia using screws. These realignment surgeries are typically conducted under sterile conditions in the operating room under anesthesia. Arthroscopic techniques may be employed, involving small incisions around the knee to visualize the joint and perform necessary interventions. Following surgery, the knee is protected with a range of motion knee brace to facilitate proper healing and alignment.
Patients are administered painkiller medications to alleviate discomfort, while regular icepacks are applied 4 to 5 times a day to reduce swelling. The operated leg is kept elevated to further diminish swelling and pain. Patients utilize a knee brace for support and mobilize in a non-weight bearing manner with a pair of elbow crutches for 4 to 6 weeks. They are instructed in exercises to be performed while lying in bed or sitting in a chair. Patients receive guidance regarding dos and don'ts during their recovery period. Additionally, regular physiotherapy sessions are essential for knee strengthening, regaining full knee mobility, and stabilizing the patellofemoral joint, facilitating a swifter recovery process.
The surgery for patellofemoral joint instability carries potential risks and complications. These include the loss of ability to extend the knee, recurrent dislocations or subluxations, arthrofibrosis characterized by the formation of thick fibrous material around the joint, persistent pain, swelling, and the development of blood clots in the legs.
Address
8/92, Sector 8, Ismailganj, Indira Nagar, Lucknow, Uttar Pradesh 226016
Monday to Friday
10am - 8pm
Appoinments
+91 - 8840223370