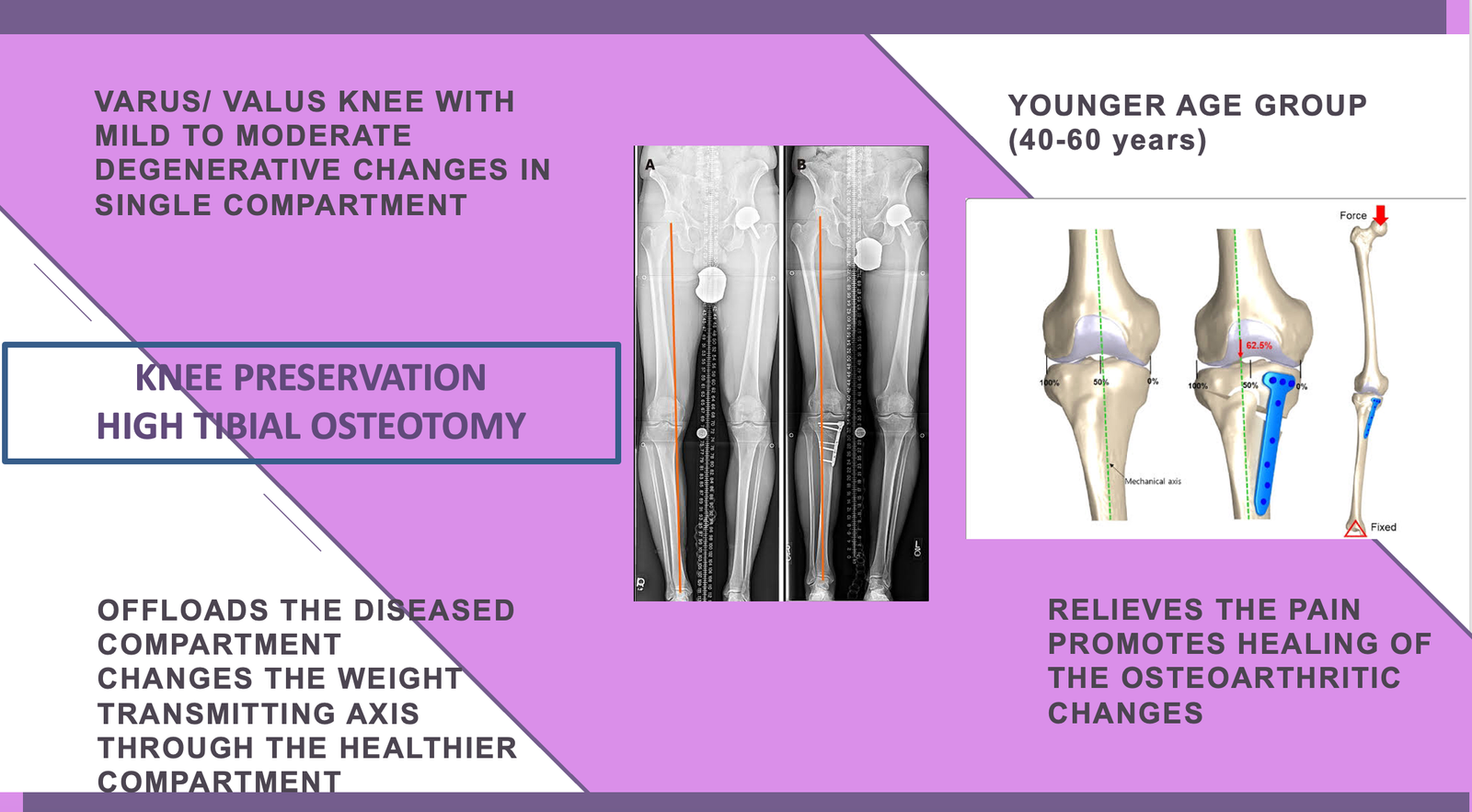
High tibial osteotomy is surgical procedure which aims to correct a varus deformation of knee joint with medial compartmental osteoarthritis.

HTO is recommended in a middle aged paitient with medial knee arthrosis with gross varus deformity, with good range of motion and without ligamentous instability.
Ideal candidates for knee osteotomy typically include those who:
Experience mild to moderate arthritis affecting one side of the knee, with minimal damage on the other.
Fall within the age range of 40 to 60 years.
Maintain a healthy weight.
Demonstrate good knee mobility, capable of full extension and at least 90-degree flexion.
Endure significant arthritis pain triggered by activity or prolonged standing.
Desire to maintain an active lifestyle and are committed to a thorough post-surgery physiotherapy regimen.
Can utilize crutches and adhere to limited weight-bearing for 6 to 8 weeks following the procedure.
Before knee osteotomy surgery, the surgeon conducts a detailed medical history review with the patient, including recent knee treatments. Both knees undergo thorough examination, along with assessments of the spine, hips, and ankle joints. Long-leg x-rays of the lower leg while standing are recommended to assess knee deformity severity and aid in preoperative planning, including calculation of bone wedge adjustments.
Blood tests for anesthesia suitability are performed, with additional investigations such as ECG, chest x-ray, and 2D echocardiography potentially conducted based on the patient’s age and medical condition.
Preoperative CT scans and MRI of the knee may be necessary for patients with complex deformities or prior injuries. MRI scans provide insight into the condition of knee cartilage and surrounding ligaments.
Patients are educated and consented prior to surgery. The procedure is carried out under either spinal or general anesthesia, often utilizing a thigh tourniquet. Typically lasting between 1 to 2 hours, the surgery commences with marking the osteotomy sites on the leg after meticulous sterile preparation.
Some surgeons conduct a brief arthroscopic evaluation of the knee initially to assess the condition of the unaffected compartment. Any minor issues with knee cartilage or meniscus are addressed simultaneously to optimize post-surgical outcomes. Surgery proceeds only if the unaffected compartment exhibits healthy cartilage.
Following planned skin incisions, the bone is exposed, and guide wires are inserted into the tibia/femur under x-ray guidance. The size of the wedge to be added or removed is tailored to the patient's anatomy and the extent of deformity. Typically, a 1 mm wedge results in a 1-degree correction, with larger wedges providing proportionate alignment changes.
The osteotomy is performed under x-ray control, either as a closing or open wedge technique. Once completed, the cut bones are stabilized using specialized plates and screws. Alignment correction is confirmed through imaging.
Closure of the wound involves dissolving sutures and tapes, followed by sterile dressings and a compression bandage. Patients are then transferred to the recovery ward for observation.
Patients can resume eating and drinking within 3 to 4 hours post-surgery. They receive ice packs and leg elevation to mitigate knee swelling, alongside appropriate pain relief.
Antibiotics are administered only for the initial 24 hours.
Patients are encouraged to initiate ankle movement and perform static quadriceps exercises.
Mobilization begins with the aid of elbow crutches or a walker, with partial weight bearing permitted for the first 6 weeks. Knee range of motion exercises are encouraged as tolerated, and
patients are provided with a hinged knee brace for added protection.
Discharge criteria include independence in activities such as bed transfers, using the commode, safe ambulation with crutches, and negotiating stairs, typically achieved within 2-3 days post-surgery.
Wound assessment occurs at the 2-week mark, with ongoing physiotherapy conducted on an outpatient basis.
Knee x-rays are scheduled at 6 weeks and 3 months to monitor osteotomy healing, which typically begins at 6 weeks and consolidates by 3 months.
Patients may require 4 to 6 months to fully experience the benefits of their knee osteotomy surgery.
For suitable candidates with appropriate indications, osteotomy proves to be an effective procedure in alleviating pain and enhancing knee function. It can potentially postpone the necessity for knee replacement surgery. Success rates indicate that at five years post-surgery, approximately 85% of patients experience sustained function and pain relief, diminishing to 70% at ten years, and around 50% at 15 years.
Following an osteotomy, individuals can generally expect to resume sports activities within six to nine months. However, this timeline may vary based on your pre-operative activity level, the extent of knee arthritis, and the progress achieved during rehabilitation.
If your job primarily involves office-based tasks, you might be able to return to work within two to three weeks. However, if your occupation entails significant walking or heavy manual labor, your return to work may be postponed for a period ranging from 6 to 12 weeks.
An osteotomy offers a favorable prospect of postponing the necessity for a knee replacement in the future. Over time, many individuals may develop arthritis in other areas of the knee or experience arthritis progression within the same compartment. In such cases, a total knee replacement may be necessary.
Typically, individuals undergoing an osteotomy often require removal of the plates, typically within one to two years post-operation. This procedure is conducted as a day operation with minimal recovery time. Removal of the plates at this stage is deemed safest to avoid any potential interference with future treatments or surgeries.
Following an osteotomy, it's common for individuals to experience some discomfort for 3-4 weeks, typically manageable with oral medication. As the osteotomy site fully heals, most arthritis-related pain symptoms tend to improve significantly, as weight is distributed onto the healthier cartilage of the unaffected compartment.
Potential risks or complications following knee osteotomy may include: swelling, stiffness, persistent pain, vascular or nerve injury, deep vein thrombosis, infection, non-union of the osteotomy site, implant failure, fractures near the osteotomy, ongoing arthritis progression despite the procedure, and potential future need for knee replacement.
High tibial osteotomy is surgical procedure which aims to correct a varus deformation of knee joint with medial compartmental osteoarthritis.
HTO is recommended in a middle aged paitient with medial knee arthrosis with gross varus deformity, with good range of motion and without ligamentous instability.
Ideal candidates for knee osteotomy typically include those who:
Experience mild to moderate arthritis affecting one side of the knee, with minimal damage on the other.
Fall within the age range of 40 to 60 years.
Maintain a healthy weight.
Demonstrate good knee mobility, capable of full extension and at least 90-degree flexion.
Endure significant arthritis pain triggered by activity or prolonged standing.
Desire to maintain an active lifestyle and are committed to a thorough post-surgery physiotherapy regimen.
Can utilize crutches and adhere to limited weight-bearing for 6 to 8 weeks following the procedure.
Before knee osteotomy surgery, the surgeon conducts a detailed medical history review with the patient, including recent knee treatments. Both knees undergo thorough examination, along with assessments of the spine, hips, and ankle joints. Long-leg x-rays of the lower leg while standing are recommended to assess knee deformity severity and aid in preoperative planning, including calculation of bone wedge adjustments.
Blood tests for anesthesia suitability are performed, with additional investigations such as ECG, chest x-ray, and 2D echocardiography potentially conducted based on the patient’s age and medical condition.
Preoperative CT scans and MRI of the knee may be necessary for patients with complex deformities or prior injuries. MRI scans provide insight into the condition of knee cartilage and surrounding ligaments.
Patients are educated and consented prior to surgery. The procedure is carried out under either spinal or general anesthesia, often utilizing a thigh tourniquet. Typically lasting between 1 to 2 hours, the surgery commences with marking the osteotomy sites on the leg after meticulous sterile preparation.
Some surgeons conduct a brief arthroscopic evaluation of the knee initially to assess the condition of the unaffected compartment. Any minor issues with knee cartilage or meniscus are addressed simultaneously to optimize post-surgical outcomes. Surgery proceeds only if the unaffected compartment exhibits healthy cartilage.
Following planned skin incisions, the bone is exposed, and guide wires are inserted into the tibia/femur under x-ray guidance. The size of the wedge to be added or removed is tailored to the patient's anatomy and the extent of deformity. Typically, a 1 mm wedge results in a 1-degree correction, with larger wedges providing proportionate alignment changes.
The osteotomy is performed under x-ray control, either as a closing or open wedge technique. Once completed, the cut bones are stabilized using specialized plates and screws. Alignment correction is confirmed through imaging.
Closure of the wound involves dissolving sutures and tapes, followed by sterile dressings and a compression bandage. Patients are then transferred to the recovery ward for observation.
Patients can resume eating and drinking within 3 to 4 hours post-surgery. They receive ice packs and leg elevation to mitigate knee swelling, alongside appropriate pain relief.
Antibiotics are administered only for the initial 24 hours.
Patients are encouraged to initiate ankle movement and perform static quadriceps exercises.
Mobilization begins with the aid of elbow crutches or a walker, with partial weight bearing permitted for the first 6 weeks. Knee range of motion exercises are encouraged as tolerated, and
patients are provided with a hinged knee brace for added protection.
Discharge criteria include independence in activities such as bed transfers, using the commode, safe ambulation with crutches, and negotiating stairs, typically achieved within 2-3 days post-surgery.
Wound assessment occurs at the 2-week mark, with ongoing physiotherapy conducted on an outpatient basis.
Knee x-rays are scheduled at 6 weeks and 3 months to monitor osteotomy healing, which typically begins at 6 weeks and consolidates by 3 months.
Patients may require 4 to 6 months to fully experience the benefits of their knee osteotomy surgery.
For suitable candidates with appropriate indications, osteotomy proves to be an effective procedure in alleviating pain and enhancing knee function. It can potentially postpone the necessity for knee replacement surgery. Success rates indicate that at five years post-surgery, approximately 85% of patients experience sustained function and pain relief, diminishing to 70% at ten years, and around 50% at 15 years.
Following an osteotomy, individuals can generally expect to resume sports activities within six to nine months. However, this timeline may vary based on your pre-operative activity level, the extent of knee arthritis, and the progress achieved during rehabilitation.
If your job primarily involves office-based tasks, you might be able to return to work within two to three weeks. However, if your occupation entails significant walking or heavy manual labor, your return to work may be postponed for a period ranging from 6 to 12 weeks.
An osteotomy offers a favorable prospect of postponing the necessity for a knee replacement in the future. Over time, many individuals may develop arthritis in other areas of the knee or experience arthritis progression within the same compartment. In such cases, a total knee replacement may be necessary.
Typically, individuals undergoing an osteotomy often require removal of the plates, typically within one to two years post-operation. This procedure is conducted as a day operation with minimal recovery time. Removal of the plates at this stage is deemed safest to avoid any potential interference with future treatments or surgeries.
Following an osteotomy, it's common for individuals to experience some discomfort for 3-4 weeks, typically manageable with oral medication. As the osteotomy site fully heals, most arthritis-related pain symptoms tend to improve significantly, as weight is distributed onto the healthier cartilage of the unaffected compartment.
Potential risks or complications following knee osteotomy may include: swelling, stiffness, persistent pain, vascular or nerve injury, deep vein thrombosis, infection, non-union of the osteotomy site, implant failure, fractures near the osteotomy, ongoing arthritis progression despite the procedure, and potential future need for knee replacement.
Address
8/92, Sector 8, Ismailganj, Indira Nagar, Lucknow, Uttar Pradesh 226016
Monday to Friday
10am - 8pm
Appoinments
+91 - 8840223370